This is our standard MRI protocol to visualize the eye and internal structures.
It contains isotropic 3D sequences, which can be used for an accurate assessment of the lesion’s dimensions and extent.
These scans are complemented with 2D sequences with a higher in plane resolution that allow for a more detailed radiological evaluation.
The scans are generally planned such that all relevant structures, e.g. tumour and adjacent optic nerve, are visible in a single slice.
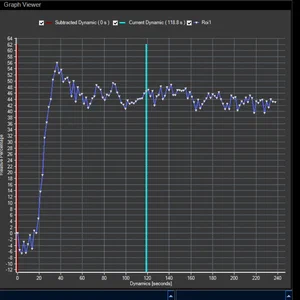
In addition to these anatomical sequences, the protocol contains functional sequences, which provide biomarkers of the lesion’s vascularity (perfusion weighted imaging) and cellularity (diffusion weighted imaging). These scans are particularly valuable for the differential diagnosis, but can also be used as an early marker of treatment response.
References
The technical rationale behind this protocol is described in
MRI of Uveal Melanoma
The images acquired with this protocol have been further described/validated in the following studies:
MR imaging characteristics of uveal melanoma with histopathological validation
Comparison of Magnetic Resonance Imaging–Based and Conventional Measurements for Proton Beam Therapy of Uveal Melanoma
MR-based follow-up after brachytherapy and proton beam therapy in uveal melanoma
Eye-specific quantitative dynamic contrast-enhanced MRI analysis for patients with intraocular masses
This protocol is furthermore the basis for our eye lid protocol and the protocol we use for the planning of ocular Proton Therapy.
Requirements
Hardware:
3 Tesla MRI
Surface (receive) coil (we use a 47mm Philips receive coil)
A support for the head (we use the MaxSupportTM wide shaped (red) variant from Medeo)
Preferably a mask/goggles for positioning of the coil (ours are made from radiotherapy thermoplastic material and Velcro)
A power injector to administer a bolus of 0.1 mmol/kg gadoterate meglumine (Dotarem) 6s after the start of the dynamic scan, followed by a 20 ml injection of isotonic saline with an injection rate of 2 ml/s
The affected eye is closed with a piece of tape and subsequently covered with a wet gauze to limit susceptibility artifacts at the air-cornea interface
Sequences:
For the 3D sequences, we use a variable refocussing angle to allow for longer echo-trains without blurring, which substantially reduces the scan time. The Philips implementation is called BrainVIEW, but other vendors have similar options (eg. SPACE on Siemens and CUBE on GE).
To increase the temporal and spatial resolution of the dynamic contrast enhancement (DCE) scan, the outer part of k-space is acquired over multiple dynamics. On Philips this is called ViewSharing, on Siemens TWIST and on GE TRICKS.
For the quantification of the perfusion data (and T1 of the tumour), we determine the B1 with the DREAM sequence.
Protocol description
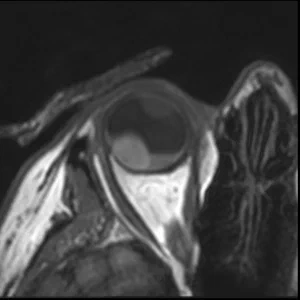
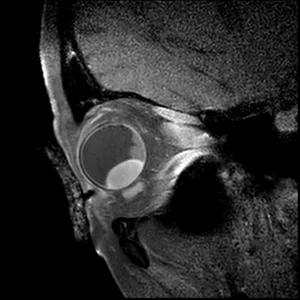
3DT1 SPIR Gd
The isotropic resolution allows for accurate 3D assessment of the lesion dimensions.
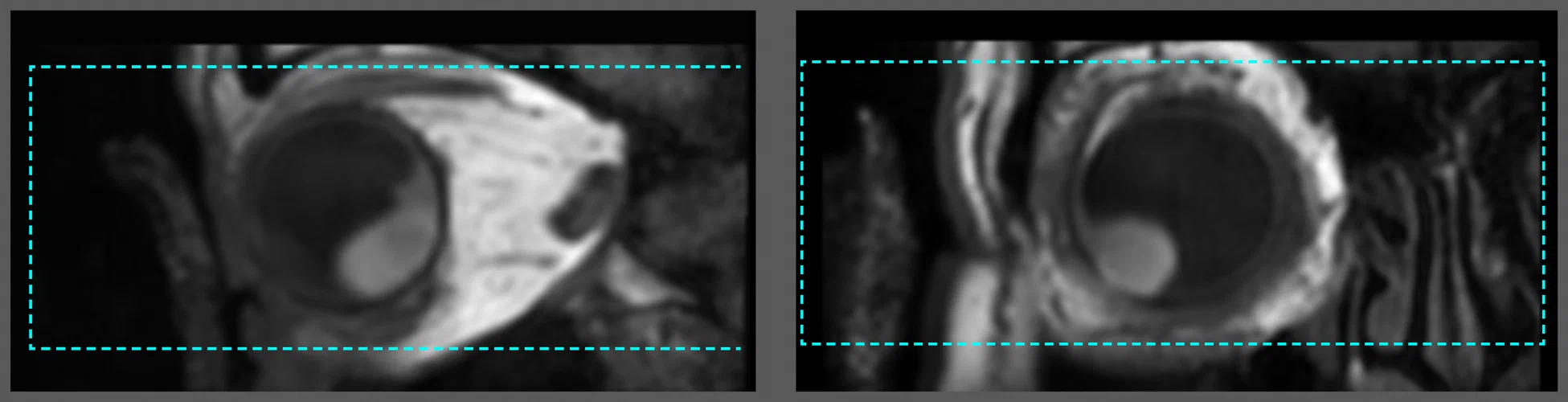
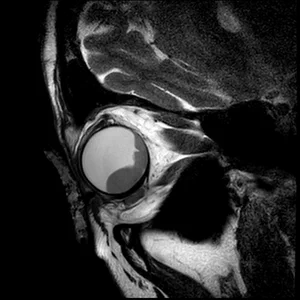
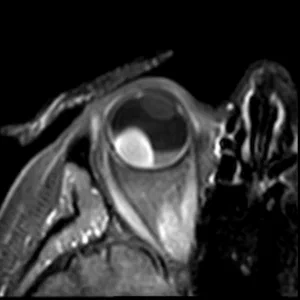
2D T2
The high in-plane resolution allows for accurate assessment of the lesions origin and relation.
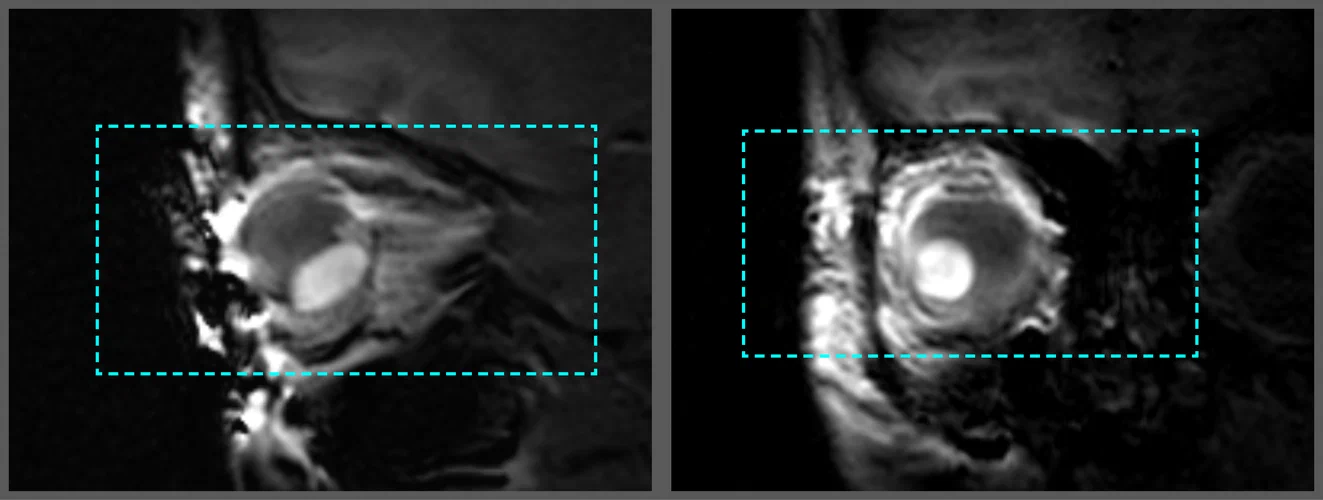
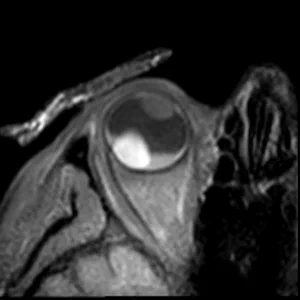
T1 & T1Gd
Contrast enhanced scans to differentiate the lesion and retinal detachment.
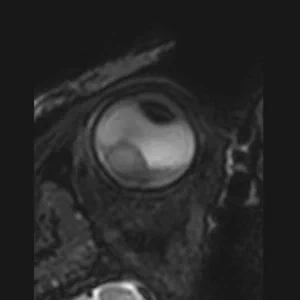
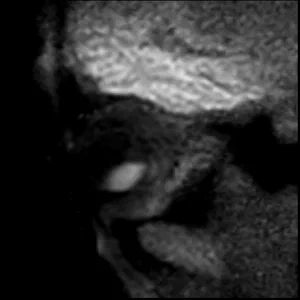
DWI ADC
Diffusion weighted imaging provides a valuable biomarker for differential diagnosis.
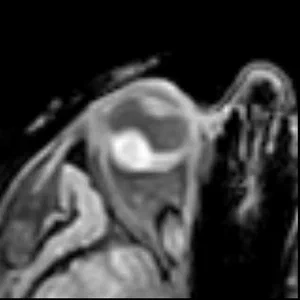
PWI
Perfusion weighted imaging provides a valuable information for differential diagnosis and of treatment response.
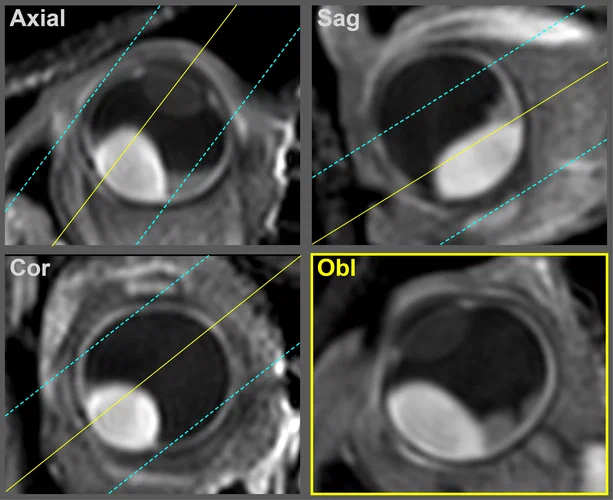
Contrast-enhanced T1 scan with high in-plane resolution
Obl
1:22
Planning
3Dtra
Main geometry for the 3D sequences. As these scans have an isotropic resolution and can thus be reformatted in any orientation, they are scanned without angulation. We plan them in the axial plane, with frequency encoding in the LR direction, to prevent fold-over artefacts.
Dyn
Same geometry as 3Dtra, but with slightly smaller FOV in the FH direction, to facilitate a higher temporal resolution for the dynamic scan.
Obl
The orientation of multi-slice scans is tailored to the location and geometry of the tumour. It is typically perpendicular to the sclera and chosen such that the lesion and associated pathology are visualized in one slice. For patients with complex pathology, e.g. both retinal detachment and optic nerve invasion, we perform these scans twice with different orientations.
Sequence details
Download the Philips examcard (release 5.6.1.2), or view the complete list of scan parameters.
3D T2
An isotropic 3D T2-weighted sequence with fat supression, allowing for a 3D visualisation of the eye and surrounding anatomy.
A T1-weighted sequence with an increased in plane resolution, allowing for a better assessment of the origin of the lesion and its relation to the surrounding anatomy.
A T2-weighted sequence with an increased in plane resolution, allowing for a better assessment of the origin of the lesion and its relation to the surrounding anatomy.
A diffusion weighted sequence with two B-values (0 and 800 s/mm2) and ADC map. This sequence is particularly useful for differentiating between benign and malignant lesions.
An isotropic 3D T1-weighted sequence with fat supression. This sequence is particularly usefull when there is suspiccion of extra-scleral tumour extensions. In these patients it provides a reference to determine if the extra-ocular component is enhancing.
Flip angle mapping sequence for T1 mapping. We use for flip angles (2, 5, 9 and 15 degrees) to accomodate the wide range of T1 values of intra-ocular masses.
3D T1-weighted sequence with fat supression after gadolinium contrast administration. This sequence is used to determine the enhancement pattern of the intra-ocular masses. The sequence parameters are the same as the 3D T1 SPIR sequence.
T1-weighted sequence with fat supression after contrast, the increased in plane resolution allows for a better assessment of the lesions relation to the surrounding anatomy.


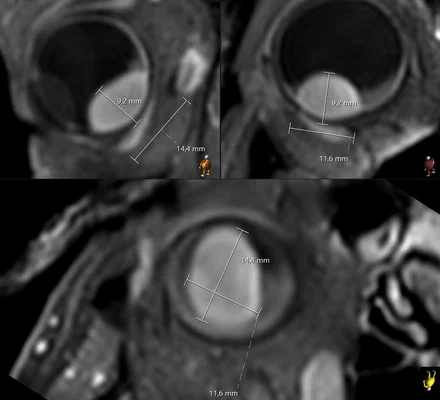 3DT1 SPIR GdThe isotropic resolution allows for accurate 3D assessment of the lesion dimensions.
3DT1 SPIR GdThe isotropic resolution allows for accurate 3D assessment of the lesion dimensions.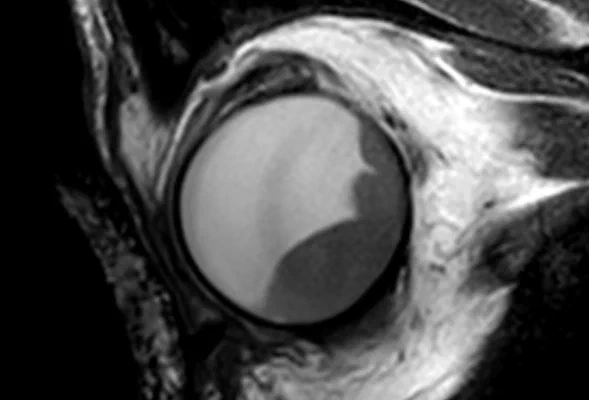 2D T2The high in-plane resolution allows for accurate assessment of the lesions origin and relation.
2D T2The high in-plane resolution allows for accurate assessment of the lesions origin and relation.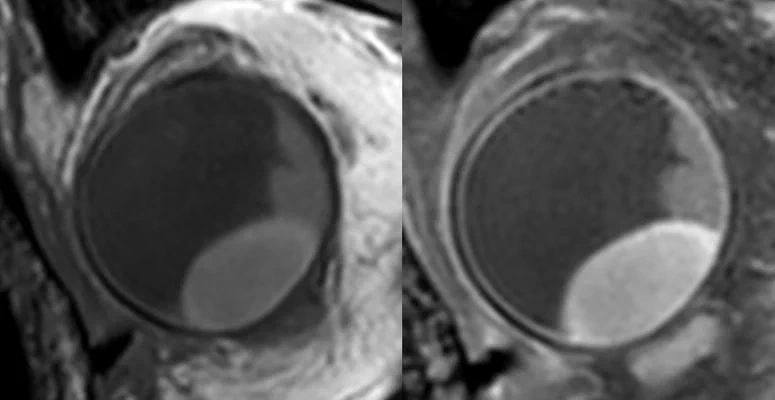 T1 & T1GdContrast enhanced scans to differentiate the lesion and retinal detachment.
T1 & T1GdContrast enhanced scans to differentiate the lesion and retinal detachment.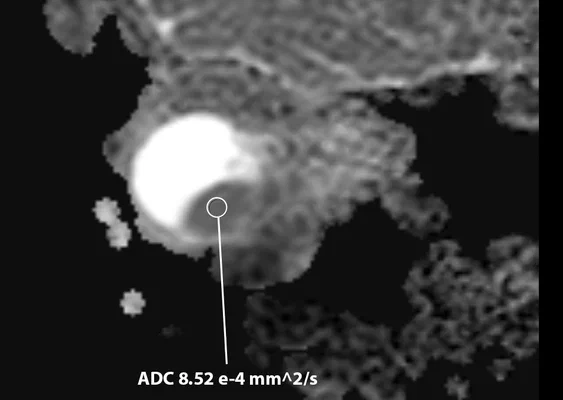 DWI ADCDiffusion weighted imaging provides a valuable biomarker for differential diagnosis.
DWI ADCDiffusion weighted imaging provides a valuable biomarker for differential diagnosis.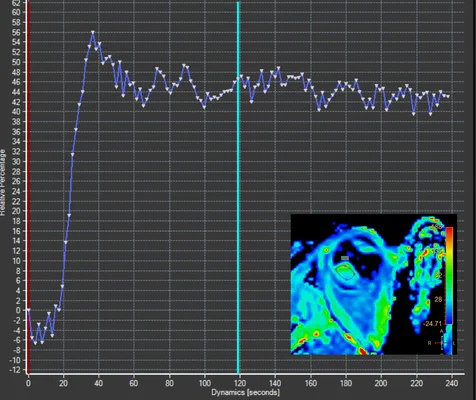 PWIPerfusion weighted imaging provides a valuable information for differential diagnosis and of treatment response.
PWIPerfusion weighted imaging provides a valuable information for differential diagnosis and of treatment response.